Date: December 15,2020
To: The state of New York and Professor Otte
From: Raynor Quiah, student at CCNY
Subject: Proposal for solving the NY ventilator shortage
Purpose
The purpose of this proposal is to gain permission to construct ventilators to solve the ventilator crisis in NY due to COVID-19. NY is running out of time and the chances of people dying are increasing. Our only hope is to mass produce these machines at a faster rate.
Summary
Professor Otte asked us to make a proposal of an engineering innovation that would benefit NYC. After some thinking, the events surrounding the COVID-19 pandemic came in mind. It completely exposed the faults of our healthcare system’s preparation in times of crisis. One of the main issues was the ventilator shortage. It was so bad that manufacturers could not keep up with the demand. Alongside that, ventilators are extremely costly. NYU Langone Health advised emergency room physicians to “think more critically” about which patients get ventilators, though New York state guidelines advise against physicians making such life-or-death decisions for their own patients. New York City Mayor Bill de Blasio told that as of April 5, the city had about 4,000 patients on ventilators and expected another 1,000 in the following days. The city needed 1,000 to 1,500 more ventilators to avoid running out by April 8. This is such a big number to meet in such few days. Although the crisis has calmed down as of today, a second wave seems apparent.
Professor Otte has specifically asked us to focus on NYC, but if the proposal is a success, we can use it nationally and even internationally. We need to develop a plan which would be cost efficient and rapid. So, to face it, I propose making ventilators with cheaper materials and simple functions, just enough to serve its purpose. Manufacturing a ventilator is difficult, especially during a pandemic, when supply lines are unreliable. Different designs negotiate different bargains between cost and functionality. Also, it is very invasive when used on a patient. What I have found is that we need to keep the device as minimalistic as possible. We must start using cheaper material and make fewer parts.
To meet the demands, I have estimated a cost of $5,000-$8000 per ventilator compared to a standard $20,000 each. That is a significant decrease. When it comes to the amount of time we need it is we cannot measure in hours or days, but in months. I estimate we can produce about 40,000 ventilators in a month and ramp up production to about 100,000- 200,000 per month depending on the size of the ever unstable workforce.
If this proposal is authorized, we would begin our production immediately, submitting to Prof. Otte a progress report, and a recommendation report. The recommendation report would include the details of our construction and recommendations regarding how to proceed with the distribution.
Introduction
Professor Otte asked us to make a proposal of an engineering innovation that would benefit NYC. After some thinking, the events surrounding the COVID-19 pandemic came in mind. It completely exposed the faults of our healthcare system’s preparation in times of crisis. One of the main issues was the ventilator shortage. It was so bad that manufacturers could not keep up with the demand. Alongside that, ventilators are extremely costly. NYU Langone Health advised emergency room physicians to “think more critically” about which patients get ventilators, though New York state guidelines advise against physicians making such life-or-death decisions for their own patients. New York City Mayor Bill de Blasio told that as of April 5, the city had about 4,000 patients on ventilators and expected another 1,000 in the following days. The city needed 1,000 to 1,500 more ventilators to avoid running out by April 8. This is such a big number to meet in such few days. Although the crisis has calmed down as of today, a second wave seems apparent.
Professor Otte has specifically asked us to focus on NYC, but if the proposal is a success, we can use it nationally and even internationally. We need to develop a plan which would be cost efficient and rapid. So, to face it, I propose making ventilators with cheaper materials and simple functions, just enough to serve its purpose. Manufacturing a ventilator is difficult, especially during a pandemic, when supply lines are unreliable. So, we have to accomplish 4 tasks:
- Determine how many patients are admitted to hospitals in NYC who require ventilators.
- Determine the materials which will be used to make the ventilators.
- Find a design which works as good as an expensive one while being cost effective because different designs negotiate different bargains between cost and functionality.
- Determine its distribution across the city.
In the following sections, we provide additional details about the proposed tasks, schedule, and budget, as well as our credentials and references.
Proposed Tasks
With Prof. Otte’s approval, we would perform the following six tasks to help determine the best course of action for producing ventilators.
Task 1. Determine how many patients are admitted to hospitals in NYC who require ventilators.
We need to know how many people are hospitalized due to COVID and how many of them need the ventilator. This is because we need to keep up with the demand or even be prepared with a sufficient stock. To this moment, there have 302,000 cases and 24,000 deaths. In an article by Politico, “Northwell Health, which has distributed guidelines on how to ration the critical equipment, is currently treating 3,299 coronavirus patients, nearly one-quarter of whom are on ventilators, spokesperson Terence Lynam said. He declined to disclose a breakdown of equipment on hand but said about 80 percent of the hospital system’s ventilators are in use. Northwell is only able to keep pace because it has been converting sleep apnea machines into ventilators with help from 3-D printers, and manually affixing air hoses to the breathing machines provided by the federal government, he said.” So, according to my calculations, we would need approximately 20,000 machines during the initial stages of the outbreak and gradually ramp up production.
Task 2. Determine the materials which will be used to make the ventilators.
We need materials which are extremely cheap but durable. The most viable options are plastic and aluminum which are cheap and easily shaped to whatever design is needed.
Task 3. Find a design which works as good as an expensive one while being cost effective because different designs negotiate different bargains between cost and functionality.
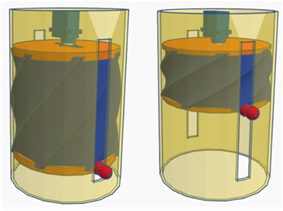
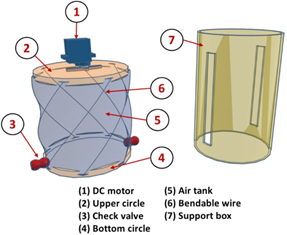
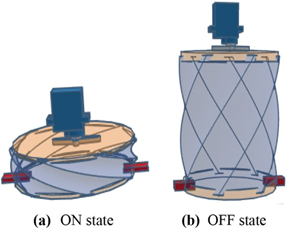
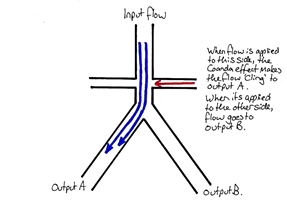
According to my research and an article by NCBI, a cheap ventilator design would comprise of a plastic air tank, two wooden or plastic circle, a bendable wire, two check valves, a DC motor, and a support box. “The motor is fixed to the center of the upper circle. In the ON state, the motor is activated, causing the upper circle to rotate in one direction. The movement of the motor causes the wire to bend. This pulls the bottom circle upwards, which pressurizes the air inside the tank.” This pressurized air is consequently directed into into a Y tube in a way that causes the Coanda Effect to make it stick to one wall and come out the opposite leg of the Y that has a mask (or airway) attached. As the lungs expand, they develop back pressure which destroys the Coanda Effect, diverting flow to the other (exhaust) leg of the Y and allowing the lungs to deflate. Once the back pressure is gone, the initial flow pattern re-establishes. This state corresponds to the inspiration phase. “In the OFF state, the motor is released. The bottom circle then moves downwards under the influence of its own weight and the release of the tension in the wire, which is restored to its initial position. Since the pressure in the lungs is higher than the pressure in the air tank, the device will draw air from the patient’s lungs. Thus, the OFF state corresponds to the expiration phase.” The cycling of ON and OFF states induces respiration. On the other hand, the movement of the bendable wire towards its initial position causes the motor to rotate in the opposite direction, so the motor can be used as a dynamo to generate electricity, thus recharging the battery.
Task 4. Distribution of the ventilators
We need to focus much of our attention towards public hospitals. It is because according to a government article 70% of admitted patients are uninsured. This means that the pressure on their banks accounts is immense. Patients who do not have a medical condition that will result in death should be at the bottom of considerations for ventilators. Patients who have a moderate risk of mortality and for whom ventilator therapy would most likely be lifesaving are prioritized for treatment. According to ventilator allocation guidelines by the state government, “… clinical assessments at 48 and 120 hours after ventilator therapy has begun are conducted to determine whether a patient continues with this treatment. Triage decisions are made based on ongoing clinical measures and data trends of a patient’s health condition.”
Task 6. Analyze our data and prepare a recommendation report
I will draft our recommendation report and upload it to Blackboard to make it convenient for classmates to help me revise it. I will then incorporate their suggestions and present a final draft of the report on Blackboard to gather any final editing suggestions.
Scheduling
On average, it takes around 2 weeks too produce a ventilator. This, of course, depends on the time taken to acquire materials, labor force and finances. As previously mentioned, we can make 40,000 ventilators in a month or 20,000 per two weeks. We can take that as our time frame. The timing will be the following:
- 2 days- allocate the budget proportionally to the number of employees needed and the cost of materials.
- 2 days-To plan out factory working conditions in terms of social distancing and proper safety equipment.
- 3 days- to start the preliminary production stages for trials of effectiveness.
- 7 days- begin mass production of the first 20,000 ventilators.
This will be repeated for the next 2 weeks to produce the other 20,000.
Budget
A budget plan outlining money allocation is provided:
- $4,000 per employee per month on the assembly line.
- $18/hr. plus hazard pay of 15% on standard 40 hour week.
- $5,000 per ventilator
- $5,000 x 20,000= $100,000 for the first 2 weeks
- $200,000 per month for 40,000 ventilators
- Total: $8,200,000/ month
Experience
I am an experienced student who has participated in numerous studies both here at CCNY and elsewhere.
Raynor Quiah, student at CCNY. I have designed many machines that would stop fare evasion on the NYC subway. I led a research which studied the effects of the pandemic on the physical and mental health on citizens. I wrote an article educating people on Airpods and whether it is wise to buy them or not.
References
Badre El Majid, Aboubakr El Hammoumi, Saad Motahhir, Ambar Lebbadi, Abdelaziz El Ghzizal. “Preliminary design of an innovative, simple, and easy-to-build portable ventilator for COVID-19 patients” US National Library of Medicine National Institutes of Health. 6 May 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7200321/
Economic Research Institute. “Ventilator Salary”.
https://www.erieri.com/salary/job/ventilator/united-states
Justin Elliott, Annie Waldman and Joshua Kaplan. “How New York City’s Emergency Ventilator Stockpile Ended Up on the Auction Block”. Propublica. 6 April 2020.
Maia Anderson. “Ventilators in critical shortage in New York City: 3 updates”. Becker’s Hospital Review. 6 April 2020.
Ventilator Allocation Guidelines.
https://www.health.ny.gov/regulations/task_force/reports_publications/docs/ventilator_guidelines.pdf